
Ranking Drug Risks Using Margin of Exposure

Drug abuse permeates society, connecting addicts, judicial systems, and policymakers in a tangled web of influence. Strategies to combat substance abuse differ across countries – some choose to attack the supply of drugs, while others attempt to curb the demand – but most of these governments agree that drug classification is a necessary foundation for regulation.
However, systems of classification can be misleading: Grouping drugs into categories can imply the comparability of harm, which is not always the case. And the panels of politicians that establish these categories and rank drugs accordingly have been criticized for sometimes inserting personal bias over scientific facts.
But now two researchers with the “Addiction and Lifestyles in Contemporary Europe – Reframing Addictions Project” are proposing an alternate way of classifying drugs in order to provide a greater understanding of their harm. They used a method of risk assessment to rank the harms of drugs called margin of exposure (MOE), which has been utilized previously by the U.S. Environmental Protection Agency to estimate the risks of cancer-causing compounds, but – until now – has never been used in the field of addiction.
We broke down the MOE research and examined the 10 substances involved to further understand the results of this study, some of which could have serious implications for the advancement of drug policy and harm reduction.
The MOE predicts how harmful a drug can be to human health. In its simplest form, the MOE is the result of a comparison between two different factors: the point at which a drug becomes harmful, also known as the benchmark dose, and how much of that drug a person or population is consuming – aka the estimated human intake.
Both parts of the ratio are crucial. If only the first variable is considered – a drug’s toxicity – a government may focus its resources on combating powerful and potentially dangerous drugs that perhaps not many people are using. But if only the second variable is considered – how much of that drug is consumed – then a government may waste its time fighting widely used drugs that don’t have the highest levels of harm. As a combination of the two, the MOE is able to acknowledge both and paints a comprehensive picture for policymakers of exactly how a drug is impacting society.
The lower the MOE, the more likely it is that a drug poses a risk to human health. While this may seem counterintuitive, it makes more sense when visualizing the margin aspect of the MOE as a “safety buffer” between the benchmark dose and the level of exposure. If this margin is small, that means the safety buffer – the conceptual separation between the dose at which toxicity occurs and the dose at which people are using it, on average – is also small, and therefore those exposed to the drug are more likely to be experiencing its toxic effects.
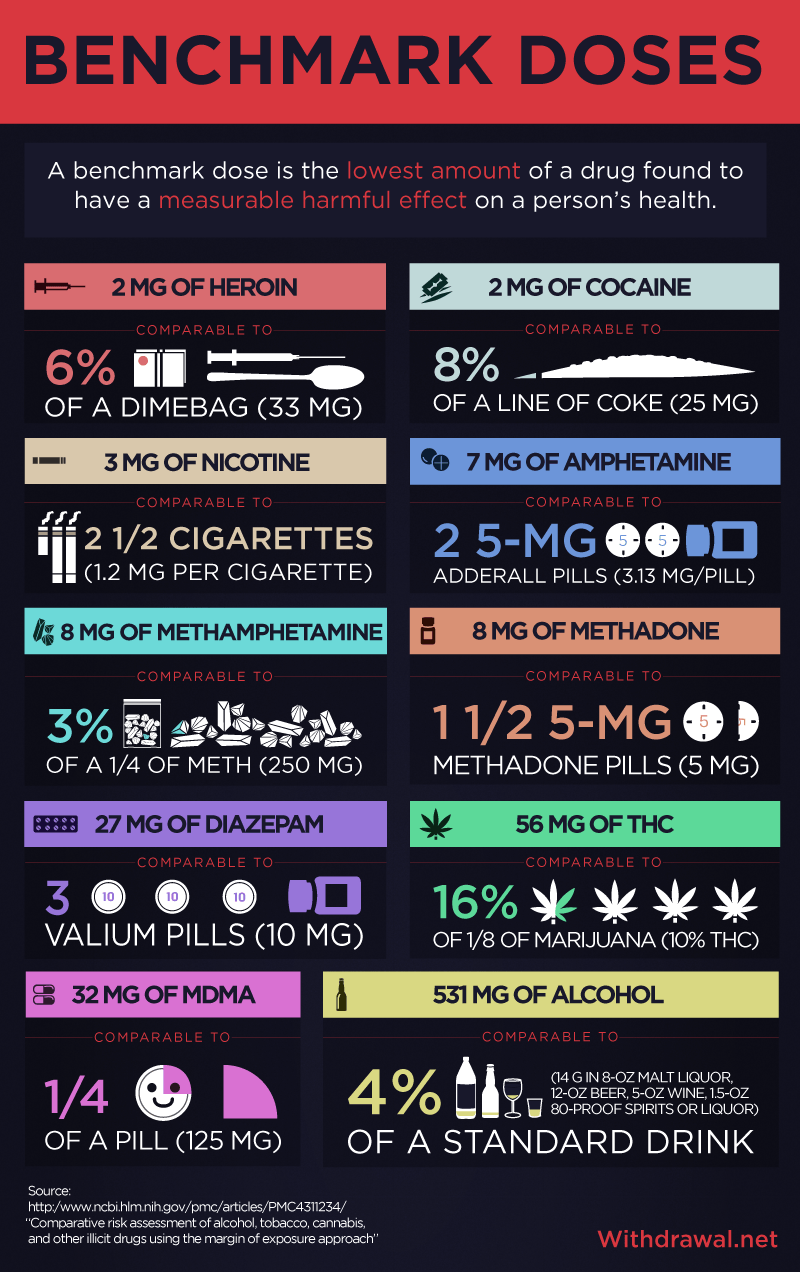
The first part of the MOE is the benchmark dose, which shows the level at which each drug becomes harmful to a person’s health. This isn’t to say that any dose under the benchmark isn’t harmful, but rather that this is the amount first observed to cause a measurable negative health effect. The health effects of lower doses either have yet to be observed or cannot yet be measured.
One of the issues researchers ran into when calculating these numbers was trying to find dose-response data for all 10 of these substances. The only available information on these drugs’ toxicity levels was LD50 data from animal experiments – the dose of a drug that killed half the animals tested – so they used those numbers to estimate benchmark doses for humans.
The toxicity of several substances – heroin, cocaine, and nicotine – is very low, ranging from 2–3 mg. Others seem much larger but remain small in comparison to the quantities normally consumed. For example, alcohol has the highest benchmark dose at 531 mg, but alcohol is normally consumed in ounces, and 531 mg is comparable to only 4 percent of a standard drink.
Not many can use less than the 2-milligram benchmark dose of heroin and stop there. The brain is programmed to keep the body alive by associating life-sustaining activities with pleasure. When drugs release this same pleasure, the brain assumes that the activity is good and encourages the body to repeat it without a second thought.
This simple process can evolve rapidly into the disease of addiction. There are a number of various resources, however, to help the addict before it’s too late. Withdrawal.net provides access to a 24/7 hotline, staffed by a team of compassionate treatment support specialists ready to provide information about programs for detox and withdrawal from drugs and alcohol – call 1-888-658-5242 today for addiction recovery options.
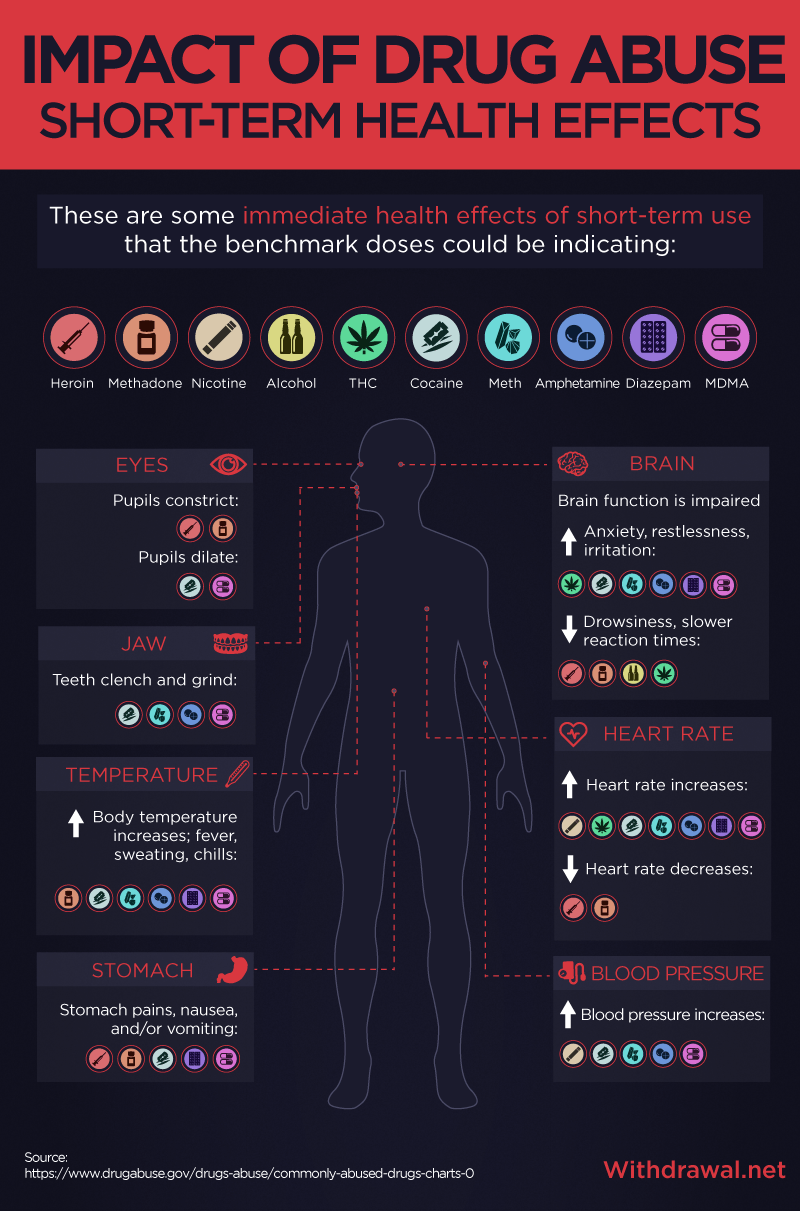
These immediate health effects occur during short-term use and could potentially be the measurable adverse health effects the benchmark doses indicate, but they say nothing about the long-term effects: disease, brain damage, or even death. The impact of drugs on an individual, not to mention a society, remains a driving force behind studies like this that attempt to illustrate the unbiased reality of toxic substances.
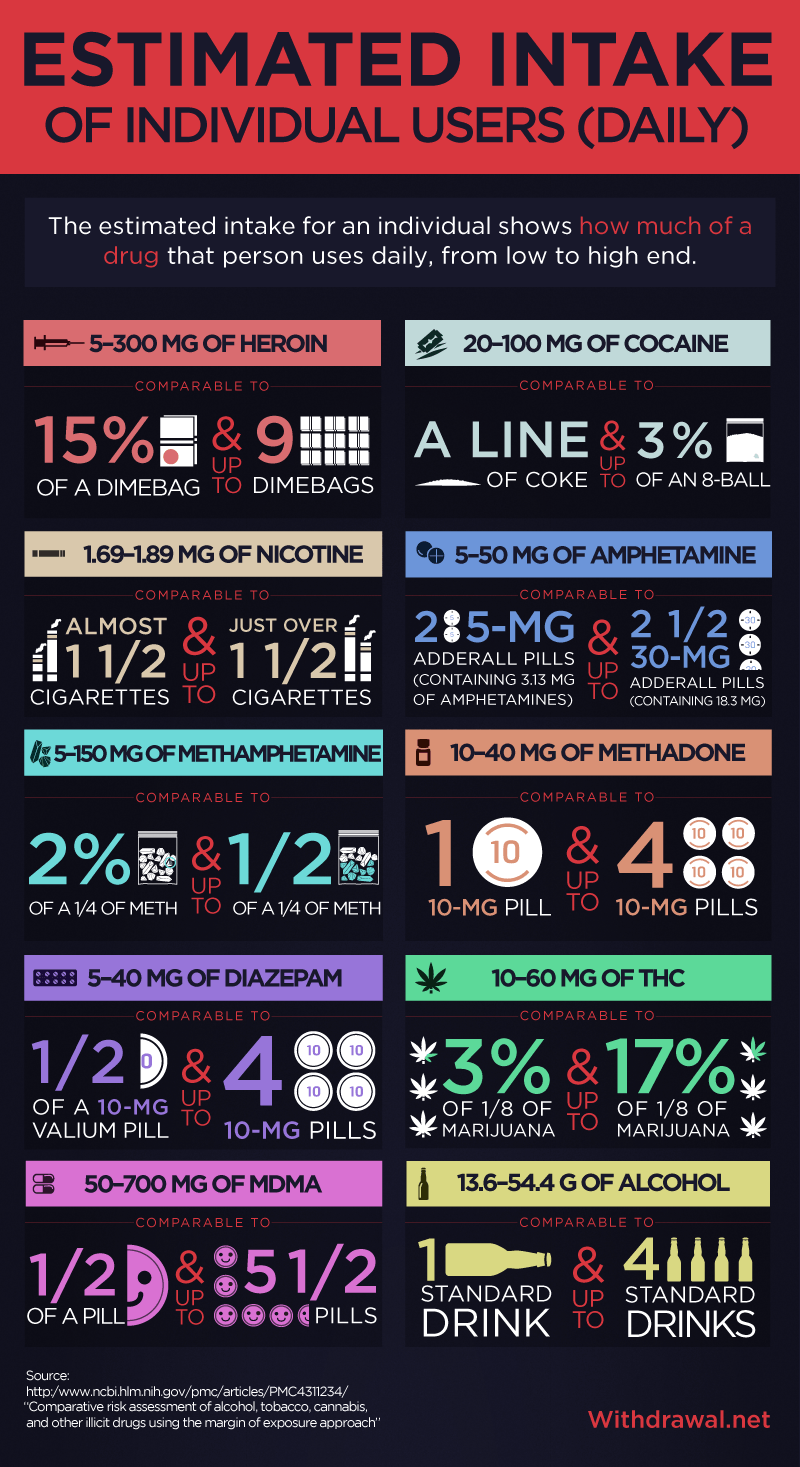
The second part of the MOE is the estimated human intake, which shows how much of a drug individuals and populations consume. In this case, researchers examined the intake of both the individual daily user and the population of Europe from low to high end.
An issue arises for researchers when estimating individual and population-wide intakes: Illegal markets make it hard to assess how much of a drug people are actually using. With such large uncertainty in the data, researchers couldn’t determine the intakes as point estimates. To fix this, they used a probabilistic calculation that takes a number of different variables into account.
The amounts consumed on a daily basis vary widely from the low to the high end of the using spectrum. A daily user of heroin consumes anywhere from 5–300 mg, while a daily user of MDMA consumes anywhere from 50–700 mg – 193 and 173 percent differences in consumption, respectively.
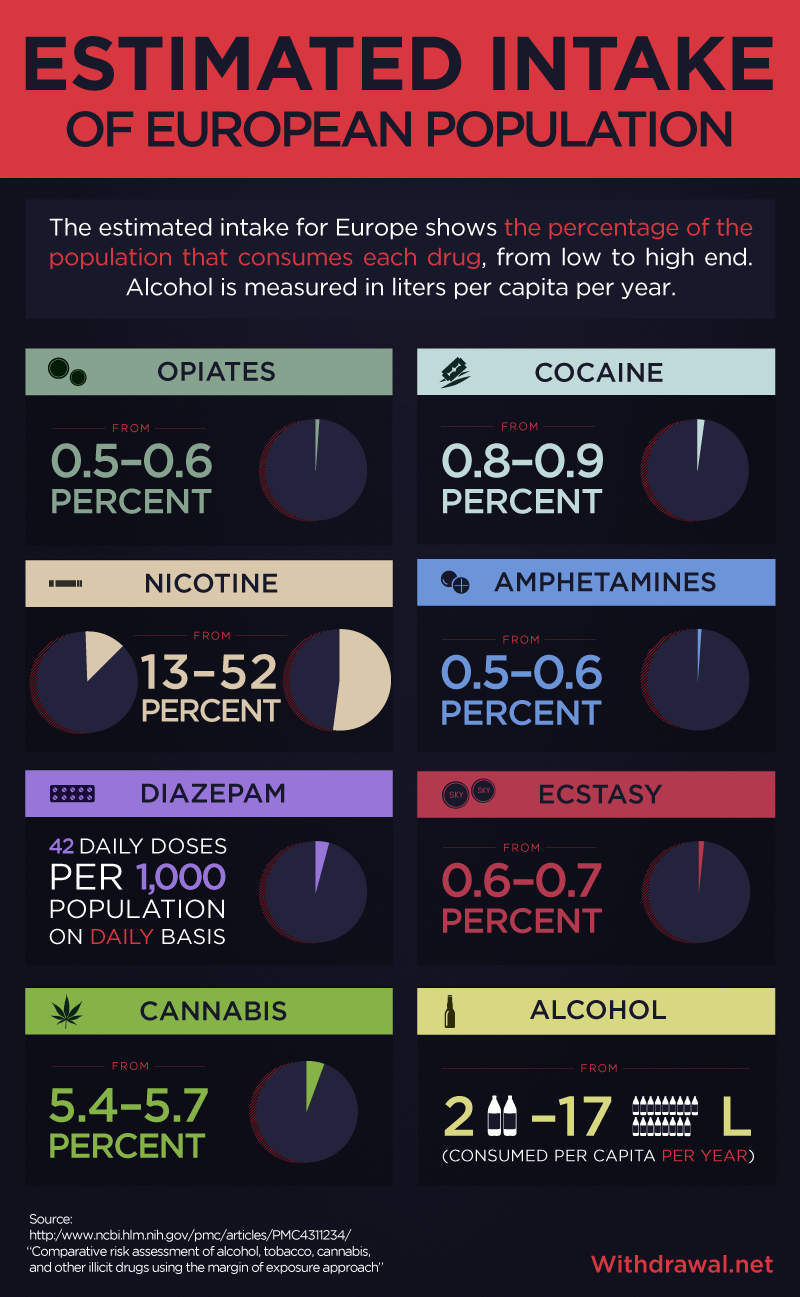
While researchers found population-based exposure data for all drugs except methadone, they ended up grouping amphetamine and methamphetamine together, as well as deviating in prevalence data for diazepam and alcohol-based on the availability of information (diazepam was measured in doses consumed per 1,000 population per day, while alcohol was measured in liters consumed per capita per year).
Cannabis is the most widely consumed illegal drug, ranging from 5.4–5.7 percent, followed by cocaine at a drop of 0.8–0.9 percent. The other illicit drugs fall below 0.6–0.7 percent. On the other end of the spectrum, nicotine’s exposure ranges from 13–52 percent, while anywhere from 2–17 liters of alcohol are consumed per capita per year. For comparison, the United States averaged 9.2 liters consumed per capita between 2008–2010.
Researchers calculated the MOE by running the benchmark doses and the estimated human intake numbers through probabilistic Monte Carlo simulations, which are computer algorithms that use repeated random samplings to obtain numerical results. Again, the lower the MOE, the more likely the drug poses a risk to human health.
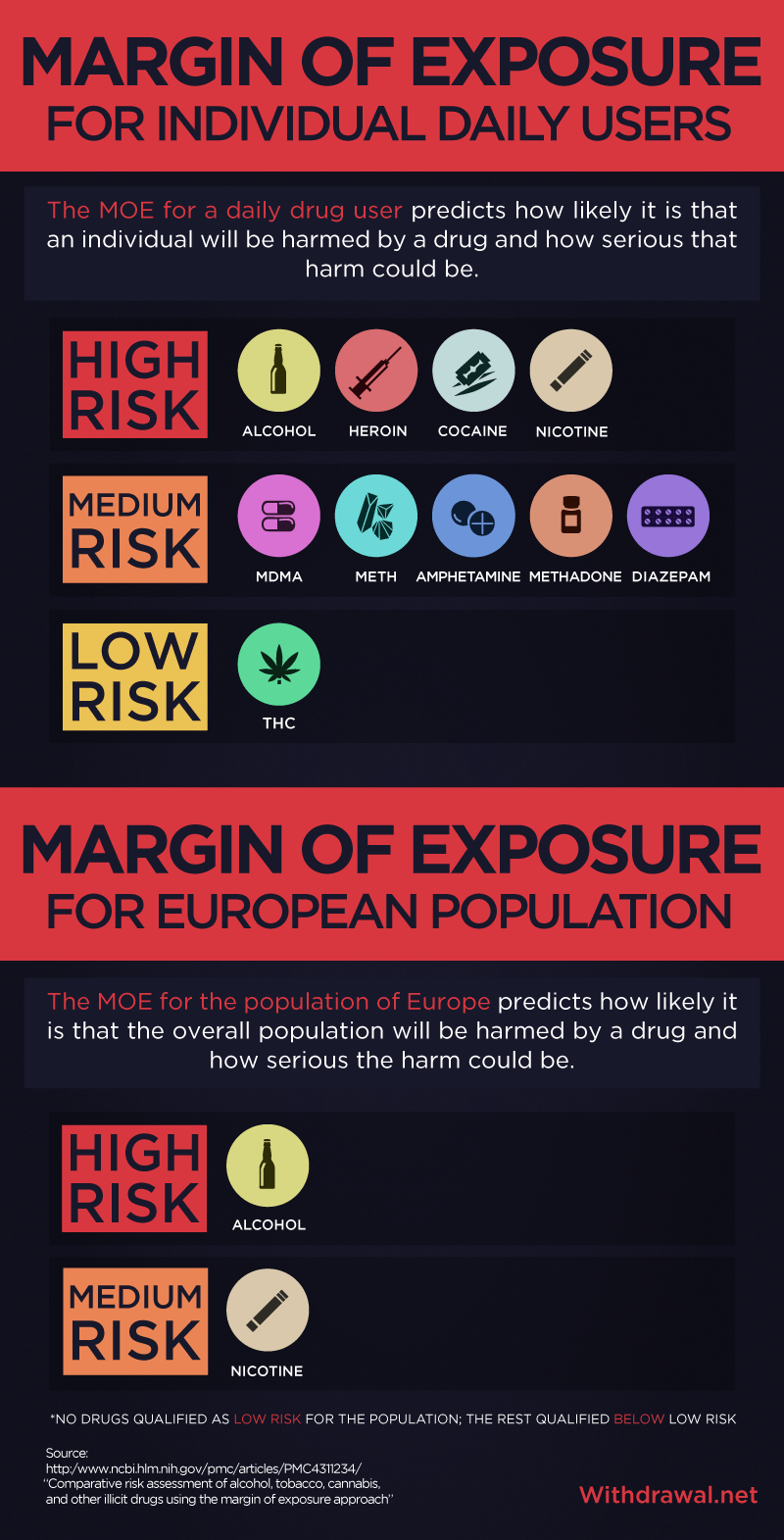
The MOE results are fascinating: For individual exposure, four substances – alcohol, heroin, cocaine, and nicotine – fall into the “high risk” category with a MOE less than 10. The rest of the compounds, save for THC, fall into the “medium risk” category with a MOE less than 100. On a population-wide scale, however, only alcohol falls into the “high risk” category, while nicotine falls into the “medium risk” category. The other substances present risks lower than the “low risk” category.
The level of intake plays a huge role, especially in the population-wide MOE. An individual who is a heavy consumer of alcohol or other drugs has an increased risk of overdose in all cases, but for society as a whole, alcohol-related deaths far outnumber drug overdose deaths. So it’s conceivable that alcohol and nicotine could have a higher MOE in the population than illegal drugs such as heroin when considering their high exposure in European society.
While it may be surprising to many as a legally obtained substance, the morbidity and mortality associated with alcohol abuse dwarfs a number of other drug types combined. If you’re concerned that compulsive alcohol is placing risks on the health of you or someone close to you, call 1-888-658-5242 to speak more about alcohol detox programs and other recovery options.
Drug Classifications in the European Union, United States, and United Nations
To embed this interactive at the following sizes, please use the codes provided below.
600px: http://embedtest.com/?hash=6d6ef627e2f88501bab5acbf0ef779c3
700px: http://embedtest.com/?hash=ba17a570e30a0c8820e2b5710ea39492
800px: http://embedtest.com/?hash=c1d60c1ad7abf049115fab59757dfaf0
1000px: http://embedtest.com/?hash=f275c1d1d8113b775eda1b39f9ffa526
Drug rankings such as the MOE approach offered by this study inform governments and the public about the relative harms of all drugs – legal and illegal.
Based on the varying levels of restriction in their drug policies, many European countries, as well as the United Nations and the United States, seem to view the abuse of illegal rather than legal drugs as a larger issue for the whole of society. However, this study’s drug ranking takes the opposite stance, suggesting that governments should prioritize risk management actions for alcohol and nicotine over other illicit drugs.
But this doesn’t mean that alcohol consumption poses a higher risk to an individual than heroin use. Many risks associated with using substances come from the inherent hazards of the using environment, which this study couldn’t measure.
Also, while THC’s low level of risk suggests that the risk of cannabis may have been overestimated – especially concerning the popularity of its restrictive drug policies – that’s not to say that THC poses no risk to human health. The risk assessment could only study mortality and not the long-term effects of drugs, as long-term experiments for all considered substances weren’t available. Cannabis may have low acute toxicity, but the long-term effects are understudied.
Conclusion
When a government bases its drug policy on a drug classification system, that system must accurately assess the harms associated with different drugs in order to best combat substance abuse. A truly accurate assessment starts with placing science over speculation. The MOE risk assessment method utilized in this study – while lacking complete certainty in data – could be a step toward a more holistic view of the risks of drug abuse.
According to this study, the two legal drugs that were considered have the lowest MOE and the highest health risk for the population of Europe. Legality seems to correlate with larger consumption, which has a huge effect on the MOE score. Of course, correlation doesn’t necessarily mean causation, but perhaps the legalization of drugs may invite an increase in consumption, which leads to an increase in overall health risks for a population.
It must be emphasized that every drug within the classification system presents significant harm, regardless of its category of risk. In other words, a “low” or even a “medium” calculated MOE risk shouldn’t be mistaken as a pass for unrestricted experimentation. Any substance can be harmful given the right (or wrong, as the case may be) dose.
Each of these chemicals carries the potential to alter the brain and precipitate the progression of addiction. And while addiction can be a progressive, fatal disease, a healthy recovery is possible with the right treatment. Obviously, the best way to minimize one’s MOE risk is to not use drugs and/or alcohol, to begin with.
That being said, if you or someone you know is struggling with addiction, visit Withdrawal.net today, or call the toll-free hotline at 1-888-658-5242 for more information about finding a rehab, detox, or recovery program that fits your needs.
Methodology
In estimating the comparisons between benchmark doses and individual intakes with recognizable quantities of drugs, we consulted various sources to determine these quantities.
For example, cocaine is normally ingested in lines. One line of cocaine equals about 25 mg, so if the benchmark dose is 2 mg, you would only need to consume 8 percent of a line to reach the benchmark dose. Alternately, if the average daily user ingests anywhere from 20–100 mg of cocaine, that would be comparable to 80 percent of a line – about one line – to 3 percent of an eight-ball, which equals 3.5 g.
Sources
- http://www.ncbi.nlm.nih.gov/pubmed/20148796
- http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4311234/
- http://epa.gov/oppt/sf/pubs/risk-assessment-calc.pdf
- http://www.epa.gov/oecaagct/ag101/pestlethal.html
- http://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/drugs-brain
- https://www.drugabuse.gov/drugs-abuse/commonly-abused-drugs-charts-0
- http://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/usa.pdf
- http://www.goldsim.com/Web/Introduction/Probabilistic/MonteCarlo/
Fair Use
Feel free to use the assets found on this page. When doing so, please attribute the authors by linking back to this page so that your audience can see all the elements and methodology involved.
